One of the big outstanding COVID crisis questions is „How did the medical care system get things so wrong?.” This excellent essay from Dr. Randall Bock uses personal experience and anecdotes from a lifetime of primary care practice spanning rural W Virginia to big city Boston to illustrate and illuminate the sickness at the heart of modern western medicine. I first met Dr. Bock right after the recent election when he reached out to interview me about USG HHS, government contracting, and BARDA. We have had many conversations since, and I have become a fan of his work and perspective. But I had no idea of his personal history. What this essay reveals is the systemic medical system dysfunction seen throughout the US and western medicine during COVID was part of a much broader problem.
“Chemistry – well, technically chemistry is the study of matter. But I prefer to see it as the study of change…. But that’s all of life, right? It’s just the constant, it’s the cycle…. It is growth, then decay, then transformation. It is fascinating. Really.” — Walter White, Breaking Bad
Like Walter White, I started as a chemistry major. During medical school summer breaks, I taught organic chemistry at Yale. That subject (which for most premeds involved “rote” memorization) is better tackled gleaning structure; finding coherence in complexity; crossing pathways of learning a language and mastering circuitry. I co-majored in physics as both disciplines demand clarity, logic, proof.
College, for me, had been a time of free-form exploration: fear, discovery, curiosity, and the exhilarating process of learning how to make propitious use of time with so many diversions possible. Medical school, by contrast, was a shock. I had imagined a deeper dive into science; what I found instead was regimentation: biology boot camp. The emphasis wasn’t on understanding but on discipline– on memorizing vast catalogs of facts before smartphones made the world’s knowledge a thumb-swipe away. It was a jarring adjustment. You weren’t guided to think critically so much as force-fed– like the goose in the pâté de foie gras process– stuffed with information until deemed ripe. Then tested.
Medicine talks a lot about being a science– but too often, it behaves like abstract art. And not the rigorous, rule-bound kind. It resembles Jackson Pollock: slapdash, mood-driven, open to interpretation depending on who’s paying the bill or writing the guideline. To be fair, some domains– like pathology or parasitology– offered clarity. I had professors in those fields whose lessons I still carry. The facts were the facts; the science was the science.
But in softer, more interpretive areas– especially those entangled with human behavior, hormones, or institutional consensus– medicine shifts. It gets personal, tribal, even theatrical. One moment, doctors are confidently headed in one direction; then comes a splash in the water– and the whole “school” veers. This isn’t clinical reasoning– it’s choreography, and fishy at that.
We call medicine an “art,” but that doesn’t excuse it from having structure. When medicine forgets it is grounded in science, it stops being either: good medicine or good science– let alone worthy art.
A Physician’s Unorthodox Path
My journey through medicine hasn’t followed the path most physicians walk. It’s been both more mundane and more surreal. I’ve practiced more hands-on primary care medicine—without mid-level clinicians—than any other MD in my circle (27 years running a solo outpatient office in a blue-collar town). I followed a simple principle: if you’re sick, come in; letting care come before coding (I also offered appointments).
A few years earlier, I’d stepped off the medical-academic track—turning down a Yale Psychiatry residency to spend a year doctoring in Calhoun County, West Virginia: a region of proud but impoverished, tradition-bound people, where time moved differently, and medicine meant earning trust across the chasm of an English spoken seemingly from different centuries (theirs from the previous).
Switching back and accepting a slot in Harvard-MGH’s Psychiatry, I found myself clashing with hierarchy and conformity, a theme that has dogged and defined much of my career. (For those interested, I tell the full story in On Becoming a Doctor, a chapter within my as-yet unpublished memoir.)
That restless streak—the refusal to go along just to get along—shaped everything that followed. I’ve questioned sacred cows, challenged orthodoxy, and paid dearly for it: a personally and professionally painful form of “no good deed goes unpunished”.
I have always believed that physicians (like attorneys) must serve the needs of the individuals enlisting them– not any institutional nor governmental directive (unless those happen to align). But in today’s system – far too often, the opposite has become the norm: medicine (perceptually and practically) genuflects to bureaucracies, to pharmaceutical incentives, and public health “narratives”– all wrapped in the sterile armor of “consensus”.
I’ve essentially never not said what I thought. That is the starting point for creating patient interactions’ comprising integrity; and shepherding a best pathway to health– or at the very least an accommodation to chronic disease. I practiced just outside of Boston, arguably a “medical mecca”; yet time and again, I saw patients emerge from these prestigious institutions utterly confused, unable to grasp what their physicians had explained: words spoken over the patient’s head, directed to medical students in tow. “Elite care” had failed the most basic test of communication.
One episode that has stayed with me involves a brilliant, older family friend who had had a one-day bout of delirium, likely due to an infection. The hospital– Brigham, no less– quickly slotted him into a psychiatric pathway (albeit on a medical floor, but failed to obtain acutely the most basic of tests to rule out intercurrent infection); perhaps subtly branding him as just another doddering, demented elderly man. Various medical teams seemingly hadn’t bothered to ask the right questions or listen. They didn’t grasp that this man had been attending dinners and holding his own in conversations at the highest intellectual levels. He had a life, a mind, a voice– and they ignored all of it: seeing only the outer mask of an old man’s briefly spouting nonsense.
It wasn’t the hospital that called me in, but the family, who were rightfully alarmed that he was being dismissed and misunderstood. Unpaid and unofficial, I found a disjointed set of subspecialists’ drifting by like ships in the night, each pursuing its own protocol without any unified direction or clinical narrative– or cohesive “business plan”within the chart.
Shockingly, no blood cultures had been done. I had to push to get even a urine culture ordered. They weren’t curious, merely operating in silos: ticking off non-sequitur procedures; entirely missing (and never finding) the cause of his condition. I made multiple phone calls to each of the sub- branches (pleading for a concerted effort to find the cause of his acute delirium), but could never get them together on a conference call.
Fortunately, he recovered fully (because of – or despite this medical stay). His mind is sharp as ever (but for that one day).
This experience, among many others, crystallized my growing disillusionment with a medical system that too often prioritizes protocol over patients, pushing me to question not just clinical practices but the very institutions shaping them.
Challenging Medical Dogma
My Authority Magazine bio-interview sketches the outlines of regulatory injustices’ culminating in professional tragedy – and rebirth. I grew up in a financially struggling (five of us in a 1.5 bedroom apartment) but conversationally forthright household, where my parents sacrificed to send us to private school. Asking inconvenient questions in pursuit of truth is my way of paying them respect. That paradigm led to my exposing the shakily irrational underpinnings of Zika-microcephaly in my book Overturning Zika; to dissect the institutional and semantic inflation behind autism diagnoses in my Substack (praised by Dr. Robert Malone as a “treatise”); and to push back against both the COVID panic machine and the prevailing mythologies of addiction.
These seemingly disparate medical topics are not unrelated threads. They represent stories of how external factors distort medical theory. Public health today isn’t about your health: it’s about managing perception, maintaining hierarchy, and avoiding blame. This pattern of prioritizing ideology over evidence extends beyond addiction to other medical domains.
Rethinking Addiction: A Heretic’s Approach
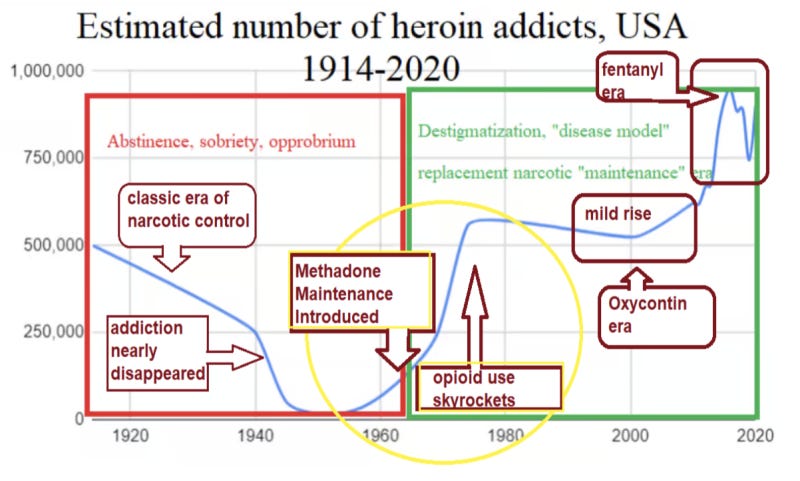
When I wrote that methadone maintenance had ignited (and continues to fan) the opioid crisis, I wasn’t merely guessing.
I had developed a successful, (multi-month-duration) slow-taper detox program– offering a pathway back to genuine sobriety, not a subscription to a lifetime of dependency, via replacement narcotics (whether methadone or Suboxone).
My patients came from all over New England– but mostly from poorer enclaves of Lynn, Chelsea, and Revere (and so often with stories sadder even than merely poverty: foster care, broken households, abuse). Many gave testimony to the joy at making progress in their lives rather than being treated with methadone clinics’ “soft bigotry of low expectations” that they would never be able to “get clean” completely. This was especially poignant on the occasion of women in early pregnancy who had begged and begged their methadone counselors and physicians to be allowed to taper to zero so they could avoid the mewling, tense, isolating detox that a methadone-babyendures on birth.
“When I first had her, she was really bad. Like, she had tremors real bad. It was the worst thing I could ever, ever see for an infant to be withdrawing.”KATIE (on methadone)
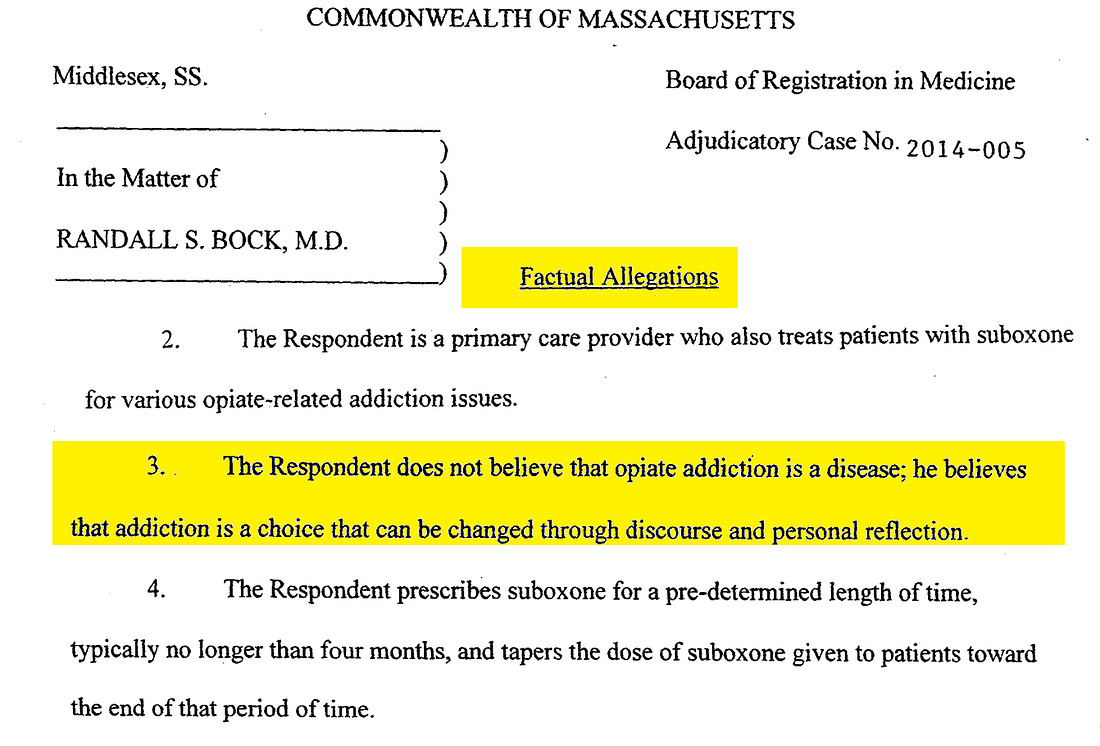
But the Massachusetts Board of Registration in Medicine (BORIM), led by proudly biasedDr. Candace Lapidus Sloane, didn’t see me as a physician committed to helping addicts reclaim their lives. It saw a heretic. My medical license was suspended, in part, based on testimony from a so-called “state expert” who never reviewed a single one of my patient charts. Moreover, she objected to my tapering narcotic addicts to sobriety (vs. “maintaining” them); while her own practice involved tapering benzodiazepine-addiction. Her entire argument amounted to quoting Nora Volkow and proclaiming, without a trace of irony, that addiction is “a brain disease by definition.” By definition (!?), that’s not science; it’s dogma.
To be fair, BORIM had its foot in the door via a patient complaint– a vindictive, vengeful, and entirely self-serving grievance from a narcotic addict who feared I might jeopardize his disability payments by helping him get sober. I never would have “snitched,” but that didn’t matter. He embellished and distorted his story, and BORIM took the word of a part-time heroin dealer over mine. It was a classic “he said, he said” (even though I had four witnesses on premises who had never noticed an untoward word from me nor any note of displeasure from him during his time in our office).
In retrospect, I was probably naïve. Maybe too self-assured. When the Board first opened an inquiry into me, I assumed its sage members would recognize that I was serious, conscientious, even thoughtful about addiction treatment. I had just finished writing Withdraw to Freedom: Navigating the Addiction Maze, which existed in manuscript form. I believed– wrongly– that reading it would reassure them. Instead, it had the opposite effect.
BORIM leadership treated the book as a smoking gun. My core sin? I didn’t believe addiction was a “disease.” The Board’s own summary got even that wrong: I didn’t merely propose “discourse and reflection.” I implemented a structured, taper-based treatment protocol from the outset—gradually reducing Suboxone over months, not just “toward the end.”
Patients came in grieving, broken, often self-destructive—and many left restored. Addiction isn’t Type I diabetes. People fall into despair and drug use, but they can climb back out. I saw it happen, repeatedly. Until I didn’t, 2014, my annus horribilis.
“Addiction is not a disease. We have a word for diseases– it’s diseases— and we have a word for addiction– it’s addiction. Changing the names of things may work for a moment, but ultimately the meaning catches up with them. People say, ‘Well, it is a disease because it changes your brain chemistry.’ Love changes your brain chemistry. Taking a walk in the woods changes your brain chemistry. That’s what the brain is: the brain is a router… for communicating spiritual truths to your physical body so you can experience them as a physical entity.”
That’s not denialism. That’s clarity. Addiction may be tragic, consuming, and complex– but so are many aspects of human behavior. Calling it a disease because it feels grave or because it changes the brain isn’t medicine. It’s theology in a lab coat; dogma dressed as science.
I don’t deny addiction’s complexity. But I reject its rebranding into a deterministic, pathological inevitability– as though relapse were as unpreventable as pancreatic cancer. Not every serious problem is a disease. Break your hip, and it might kill you– but we still call it an injury, a trauma, not a chronic illness.
The author of Naked Lunch (1959), William Burroughs– a dissolute scion of a wealthy family, muse to the Beat Poets, (in)advertent William Tell–wannabe wife-killer, and (of course!) a Harvard man– didn’t stumble into heroin addiction blindly. By his own account, he embraced it knowingly. Burroughs aptly called narcotic addiction a “disease of exposure.” It doesn’t arise spontaneously. It requires cultivation, distribution, and availability of the drug– “junk,” in his terms. Nobody in 1000 years of (not so Dark-) Middle Ages’ Europe suffered from heroin addiction. It didn’t exist. Some in Asia, where opium was prevalent, perhaps did. That makes narcotic addiction a condition with a historically and geographically contingent distribution– not a timeless biological disease.
Even today, addiction correlates more closely with trauma, alienation, idleness– and yes, bad choices: just like gambling, porn, or compulsive overeating– than with any pathogen or gene. And irony abounds: the same population, placed in different social and moral environments, can display wildly different addiction rates. The English and Scots-Irish stock of the Intermountain West, for instance, show nearly zero heroin addiction when Mormon, but substantial addiction rates when not. Likewise, heroin and opium abuse plagued a war-torn Southeast Asia, but plummeted when the same people– Vietnamese, Cambodian, Laotian– migrated to the U.S. and thrived in ways they never could back home. In Indochina, they were impoverished, but for opium crops – but never diseased at the molecular level. Addiction is not destiny. It is context.
Yet instead of treating narcotic addiction as a human condition (or even analogously to how it treats alcohol- or benzodiazepine- addictions: certainly with care and psychotherapy but with either abrupt or gradual detoxing completely away from the addicting substance), medicine decided (surprise!) to “medicalize” it– carving out a permanent revenue stream, wrapped in scientific jargon, enforced by regulation. I had challenged that model: arguing for autonomy; for tapering; for sober pregnancies’ leading to unaddicted babies; for personal agency; for treating the individual– not for extending dependency any longer than necessary under the guise of (a coincidently self-reimbursing) compassion. That stance put me squarely in the crosshairs.
Professional Exile and the Cost of Truth
After I overturned the Board’s first suspension in court, it reinstated my license– and then immediately suspended it again. Not because I had harmed patients, but (arguably) because I was a threat to the model: refusing to endorse the “lifetime Suboxone subscription” racket that lines the pockets of addiction “specialists.” I fought back– again– and won. But the damage had been done: years of lost income; professional exile; endless legal forays and expenses; my beloved walk-in clinic shattered and shuttered.
“Regrets, I’ve had a few”: the upheaval my family was put through; a lack of realizing a Sword of Damocles’ looming within an ideologically-driven BORIM (but how could I have known?)– however, I don’t regret my thoughts, my imperatives, my theories, and (case-by-case) my actions. I am a (pre-Covid -era) victim of thinking freely (wrongthink thoughtcrime). Conversely, my docketed Supreme Court case advocates for medical free speech– and a reversal of politicization of medical boards.
Panic as Policy: Medicine’s Failure to Learn
I see now that this pattern– of channeling physicians’ thoughts and actions through ideology rather than evidence– is everywhere. It’s not just addiction. It’s COVID. It’s autism. It’s Zika. It’s menopause. Remember Dr. Susan Love? A prominent breast surgeon with little clinical focus on hormone therapy, she helped spark a national panic over HRT in the 1990s. The ensuing hysteria– amplified by the media and medicine (via the 2002 Women’s Health Initiative (WHI) study, led by JoAnn Manson)– drove millions of women into abrupt, unmanaged menopause.
Dr. Manson two decades later called it“the most dramatic sea change in clinical medicine that I have ever seen.” Newsweek characterized the response as “near panic.”
Lost in that stampede was the simple truth: regular medical contact– especially for women on HRT– not only improved quality of life, but also enhanced early cancer detection and survival. The initial WHI findings, skewed by a cohort of older women well past menopause, ignored the benefits for younger women in early menopause– where the risks are lower, and the improvements in vitality, mood, and long-term health are significant.
It’s the same playbook we saw during COVID: a narrow risk in one demographic– exaggerated, universalized, and weaponized against everyone. The best course for the young was buried beneath panic meant for the old. We were told the science had spoken, when in fact it had only whispered– and been misheard.
They say history doesn’t repeat, but it rhymes. In modern medicine, it rhymes with silence, panic, and obedience. The fallout from that blind spot is only now being reversed. “Women live longer, feel better. The benefits are overwhelming”, said the FDA’s Dr. Marty Makary– just days ago.
“We” (in “Big Medicine„) should have known better, sooner. PS, I did – and I never changed my HRT-prescribing willingness throughout the 2000s and 2010s: as a lonely voice in the wilderness: treating individuals individually.
Big Medicine too often prefers consensus to truth. Same with autism. As I outlined in my essay Unraveling Autism’s Surge, the explosion in diagnoses isn’t just biology– it’s semantic. Funding, insurance codes, and shifting diagnostic categories, have fueled the surge in autism diagnoses. COVID followed a similar pattern, prioritizing catastrophe over calm, mandates over choice, and censorship over debate, dismissing the collateral damage– overdoses, shuttered businesses, educational collapse– as necessary.
A Call for Courage in Medicine and Beyond
What I’ve learned is this: we have too many experts, too few advocates.When O.J. Simpson went to court, he didn’t get a general counsel for society– he got lawyers just for him. We are far more innocent than he and we deserve the same and better: not groupthink; not population-level dictates. A physician (rightly) serves the patient, not the state, not the insurer, not the CDC. That was the ethic of my medical office. And for that, I was crushed.
Now, I’m still speaking out: through Brownstone; through Substack; through YouTube; through the courts, where I argued that licensing boards shouldn’t get a free pass to crush dissent under the guise of (a falsely-perceived sense of) “safety.” I’ve paid a price. But I’ve gained something more valuable: clarity.
The real public health crisis isn’t opioids, viruses, or autism. It’s cowardice. It’s the institutional refusal to say, “We were wrong.” And worse– it’s the power to punish those who do. If you’ve read this far, you already know what I mean. You’ve probably felt it. If so, I invite you to stand with me. Because the truth isn’t cheap– but it’s worth every sacrifice.
“The trouble is that …much of the application process isn’t built for honesty. Just as I once scrambled to demonstrate my fluency in D.E.I., students now scramble to script the ideal disagreement [civility test], one that manages to be intriguing without being dangerous.” Alex Bronzini-Vender
Why not admit students based on merit, and then teach them how to debate vigorously and disagree honorably? Civility has its place– on the bus, at the dinner table– but not as a gatekeeping metric for truth-seekers– and not on the debate stage whether real or metaphoric (and medical). Not when lies are on the line, personally and societally. But that’s the direction we’re heading. DEI initiatives, peer enforcement of ideological etiquette, and a shift away from academic rigor toward enforced emotional consensus are eroding the very foundations of intellectual independence.
We need a generation of physicians– and thinkers– trained not in compliance, but in courage. The future of medicine, and of liberty itself, depends on it. But liberty is eroding fast. In the UK, the benignly named Online Safety Bill grants bureaucrats sweeping authority to censor speech online in the name of “protection.” In reality, it’s protection for power– protection from dissent. Echoing Elon Musk, Hananya Naftali noted, “They don’t ban hate speech. They ban speech they hate.”
When we can no longer tell the truth– about medicine, about biology, about addiction, about risk then all we have left are narratives. And those who challenge the narrative become the enemy. We must continue with clarity, courage, and a commitment to serving the individual– not the system. That is the only path forward. The only oath that matters.