
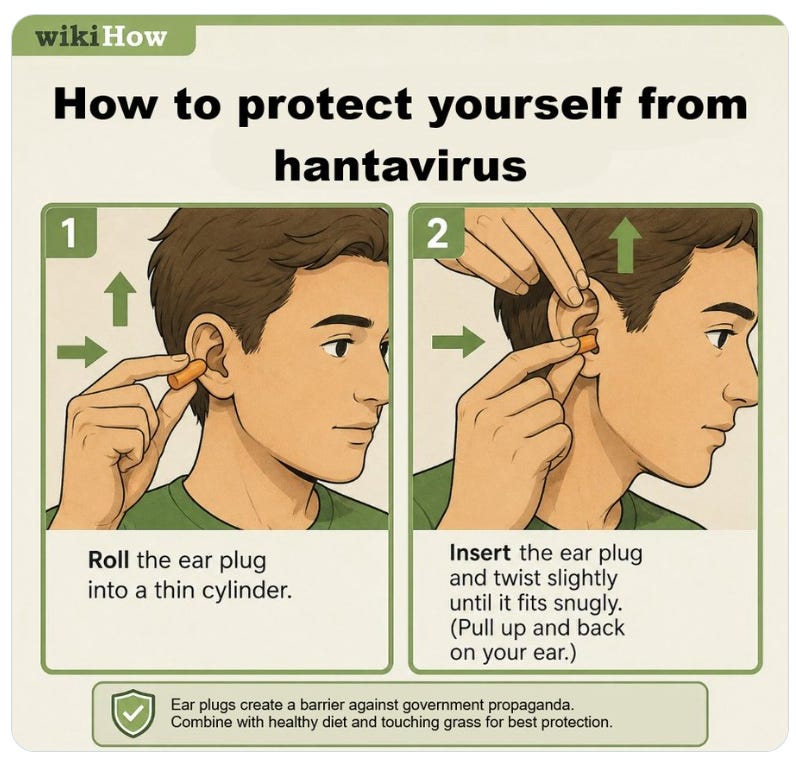

Seriously.
Mainstream Media has gone from Hantavirus to Norovirus to Meningitis (in the UK) to Ebolavirus within one month.



Dr Robert Malone: Wielkiej uczoności głupiec czy zdrajca Prawdy ?
Mirosław Dakowski, 6 marca 2026
Z Viki: Dr Robert Malone wraz z zespołem opracował technologię mRNA w 1988, a rok później złożył patent na swój wynalazek. W czasie plandemii stanowczo punktował jej absurdy i szkodliwość.
Doktor Robert Malone, poza tym że był świetnym naukowcem, a nawet uczonym, był i jest amerykańskim publicystą politycznym. Od dość dawna umieszczałem jego Friday Funnies oraz Sunday Strip.
Ukazywały one w postaci wymownych MEM-ów – jak sądzę prawdziwie – życie i spory polityczne w USA. Było to wesołe, ostre, ale i przekonujące.
Z tym większym zaskoczeniem ale i bólem zauważyłem, że po ostatnim brutalnym ataku władz Izraela oraz prowadzonego przez nich na smyczy Trumpa [USA] na Iran – i to w czasie prowadzonych z władzami Iranu negocjacji [!!!] – Malone stanął po stronie tych międzynarodowych bandytów.
Na początku myślałem, że to może wpadka, jednorazowe poślizgnięcie się. Ale okazuje się, że w następnym tygodniu powtarza prostackie, wręcz chamskie ataki na Iran oraz usprawiedliwia agresorów.
Można przecież zapytać: Ilu spośród 300 milionów dorosłych Amerykanów uważa że Iran im zagraża?
Czy tak logicznie myślący naukowiec jak Robert Malone nie widzi odpowiedzi na to pytanie?
Ze smutkiem informuję więc, że odtąd jego MEM-ów piątkowych i niedzielnych nie będę umieszczał.
Dr. Robert W. Malone Feb 27, 2026


[Brag i bragging – oznaczają przechwalanie się. asshat, arsehat – dupek; arogant. md]



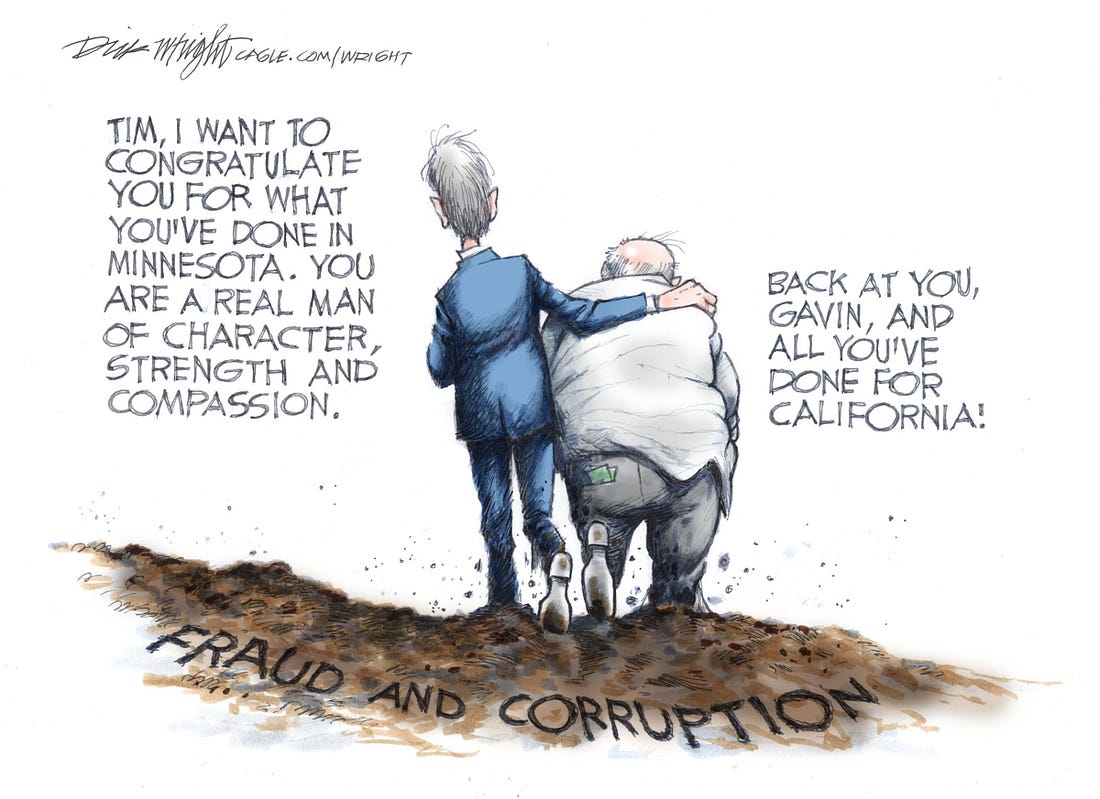
He doesn’t govern so much as he tours. Every microphone becomes a spotlight, every press appearance a carefully staged scene, while the state he’s supposed to manage simmers on the back burner. Wildfires flare, water systems creak, rolling blackouts hum — but those aren’t cues for him, just background noise to the next photo op. The problem with living under the lights is that they don’t just illuminate, they expose. When you build a career on visibility, every crack shows in high definition. The real work waits in the wings while the roadshow rolls on, polished optics and soundbites front and center. In a world where attention is currency, overexposure is the cost.
He stands in the limelight while backstage, the theater is ablaze.
- from: Worlds Amiss

Malone News is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
Thanks for reading Malone News! This post is public so feel free to share it.

Dr. Robert W. Malone Feb 22, 2026





Malone News is a reader-supported publication. To receive new posts and support our work, consider becoming a free or paid subscriber.
Thanks for reading Malone News! This post is public so feel free to share it.


That’s it for now.
| Dr. Robert W. Malone Feb 20 |
Schumer is dirtying the American flag – by using it as a rug… again.
Politicians and diapers should be changed frequently, and for the same reason.”
As long as there are final exams, there will be prayer in schools.
Politics is the second oldest profession and it bares a striking resemblance to the first oldest profession.
Just to show you how youthful I am, I am going to campaign in all thirteen states.
Attributed to either George Bernard Shaw or Oscar Wilde
Malone News is a reader-supported publication. To receive new posts and support our work, consider becoming a free or paid subscriber.
Thanks for reading Malone News! This post is public so feel free to share it.
You’re currently a free subscriber to Malone News.
For the full experience, upgrade your subscription.
| DR. ROBERT W. MALONE FEB 15 |
In my younger days, that would be me – and it certainly was my mother!
Not so much now – we avoid all things sugar as much as possible.
The benefit? No more pre-diabetes and other chronic diseases.
For the past four years, we have kept off the 40-50 pounds we each lost. How we do it isn’t rocket science…



With this harsh winter, farmers need all the support they can get. Which is why Celine Dion is doing her bit by:
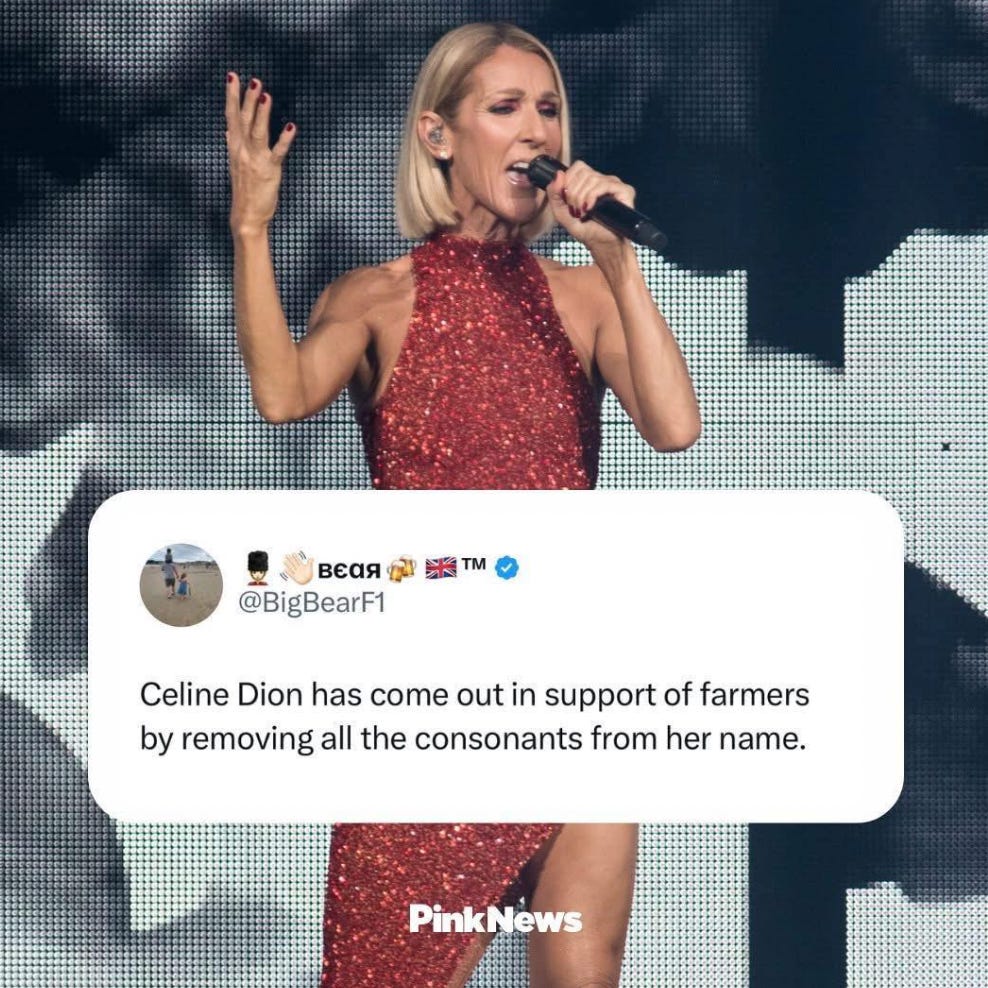
EIEIO




Zoom. Zoom.
Malone News is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
Thanks for reading Malone News! This post is public so feel free to share it.
| DR. ROBERT W. MALONEFEB 13 |

I had to look this one up…


BREAKING NEWS!
The FBI has made its first arrest in the Epstein case!





Pro tip: Searching for „X” for Valentine’s Day memes is not a good idea.
Not xure when my eyes will recover… Yuck!
Malone News is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
Thanks for reading Malone News! This post is public so feel free to share it.

In the United Lounge, getting ready to fly back from Austin – it has been a long week with a lot of fun and exciting stuff happening. More on that later!
Stay tuned!
| DR. ROBERT W. MALONE FEB 8 |

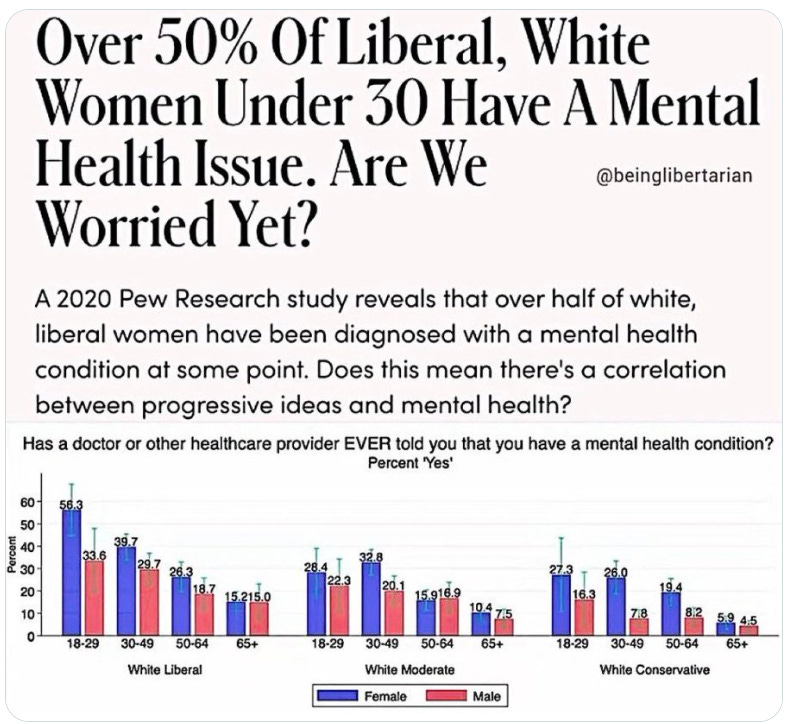
liberal women report lower levels of happiness and life satisfaction compared to conservative and moderate women. According to the 2024 American Family Survey, only 12% of liberal women aged 18–40 said they were “completely satisfied” with their lives, compared to 37% of conservative women.
Similar disparities were found in mental health and feelings of loneliness, with liberal women being the least happy and loneliest group in the survey.
A 2020 Pew Research Center study found that 56% of white liberal women aged 18–29 had been diagnosed with a mental health condition by a medical professional, more than double the rate among conservative women (27%) in the same age group.



U nas się mówiło: Proszę najpierw ten pan z syfilisem, a potem pani z zastarzałą
rzeżączką..]
============

Malone News is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
Thanks for reading Malone News! This post is public so feel free to share it.
A true COVID hero!
My Friend Brad – in 2023.
If you enjoy Malone News, share it with your friends and earn rewards when they subscribe.
| DR. ROBERT W. MALONE FEB 6 |




Malone News is a reader-supported publication. To receive new posts and support our work, consider becoming a paid subscriber.




Thanks for reading Malone News! This post is public so feel free to share it.




“You be nice chicken”
Luckily for us, we don’t own this kind of emu…

It turns out the Charleston, WV, is way colder than Virginia!
Glad to be driving home today!

| DR. ROBERT W. MALONE FEB 4 |

We have all heard the phrase “eat your greens.” Well, it turns out that some greens are healthier than others. Probably at the top of the list as the healthiest produce you can eat is broccoli.
Broccoli’s reputation as a cancer-fighting food isn’t based on vague “antioxidant” claims, but on a few very specific compounds and how the body uses them. The most important one is sulforaphane. Interestingly, broccoli doesn’t store sulforaphane in ready-to-use form. Instead, it contains a natural compound called glucoraphanin, which converts to sulforaphane when broccoli is chopped, chewed, or sprouted. That change happens with the help of a natural enzyme found in raw broccoli, and it’s especially active in young broccoli sprouts.
Once sulforaphane is formed, it works less like a vitamin and more like a signal. It switches on the body’s own cleanup and defense systems, helping cells neutralize and clear out potentially harmful substances before they can damage DNA. Rather than chasing damage after it happens, sulforaphane helps the body stay ahead of the problem, which is why it has attracted so much attention in cancer prevention research.
Sulforaphane also appears to help keep cell growth in check. In studies, it has been shown to slow down the growth of abnormal cells and, in some cases, help trigger the natural process that tells damaged cells to shut themselves down. Notably, it tends to place more stress on unhealthy cells than on normal ones. Researchers have also found that it can influence how genes are turned on and off, helping cells that have gone off course behave more normally again.
Beyond sulforaphane, broccoli contains other helpful plant compounds. Some support healthy hormone balance – like DIM, which is why cruciferous vegetables are often studied in relation to breast and prostate health.

Broccoli also provides vitamins and minerals that support immune function and DNA repair. These nutrients play supporting roles, but together they help explain why broccoli, and especially broccoli sprouts, consistently show up as standout foods in long-term health research.
In short, broccoli’s cancer-fighting reputation is grounded in biochemistry, not myth. It does not “kill cancer” outright, but it supports detoxification, epigenetic regulation, hormonal balance, and cellular self-repair in ways that plausibly reduce cancer risk over time. It is food functioning less like a vitamin pill and more like a biological signal, nudging the body toward resilience rather than reacting after damage is done.
I know people get tired of hearing that they should buy organic produce. But here’s the thing about growing broccoli: everything, every plant-loving insect loves some broccoli. As a gardener, I have never had a broccoli crop that wasn’t attacked by aphids. No matter what region of the country we lived in. Due to insect pressure, broccoli often receives multiple insecticide applications each season, sometimes weekly during periods of high pest pressure. These can include synthetic pyrethroids, neonicotinoids, spinosad, and diamides.
Broccoli consistently ranks in the middle to upper tier for insecticide residues among vegetables. It is not as residue-heavy as strawberries or leafy greens like spinach, but when tested for residue, it has more insecticide residue than root crops or fruits with thick peels.
In contrast, broccoli sprouts almost never show pesticide, herbicide, or insecticide residues in monitoring data. They are grown indoors, harvested quickly, and avoid the entire insect-control cycle. From both a nutritional and residue-exposure standpoint, sprouts concentrate the benefits while largely skipping the downsides. However, finding broccoli sprouts being sold in a conventional grocery store can be problematic, to say the least.
Cooking broccoli doesn’t destroy its healthy compounds so much as it changes how well your body can use them. The key protective compound, sulforaphane, is made from a precursor called glucoraphanin, which is fairly heat-stable. Light steaming preserves most of it, and even roasting or stir-frying doesn’t do much damage. Boiling is the main problem because glucoraphanin can simply leach into the cooking water. What cooking reliably destroys is the enzyme needed to convert glucoraphanin into sulforaphane. So cooked broccoli may still contain the raw materials, but much less of the finished, beneficial compound.
This same issue shows up in supplements. Most broccoli seed extract supplements don’t contain sulforaphane itself, but rather glucoraphanin from broccoli seeds. Some supplements rely on gut bacteria to do the conversion, which works well for some people and poorly for others.
Higher-quality products often include a natural enzyme source, such as mustard seed, to improve conversion reliability. When a label talks about “sulforaphane potential,” it usually means the precursor, not sulforaphane itself.
The key thing in mustard seed that boosts bioavailability is myrosinase.
Myrosinase is a natural plant enzyme that acts like a switch. On its own, broccoli (and broccoli supplements) mostly contains a precursorcompound, not the finished, protective one people care about. Myrosinase is what flips that precursor into its active form. Raw mustard seed happens to be one of the richest, most reliable sources of active myrosinase, and unlike broccoli’s enzyme, it survives storage and processing surprisingly well.
So broccoli seed extract or naturally sourced glucoraphanin supplements also need to contain Myrosinase, often derived from mustard seeds.

Above is the particular brand that Robert and I take (this is not a paid product endorsement), but a warning – broccoli seed extract isn’t cheap. The product is third-party tested:
Although glucoraphanin can be made in a lab, it’s too complex and expensive to produce for everyday supplements. Nearly all consumer products use plant-derived extracts instead. In real life, the limiting factor isn’t how much glucoraphanin you consume, but whether it gets converted. Cooked broccoli can still help when paired with foods like mustard or raw cruciferous vegetables, while supplements vary widely in how well they address this conversion step. Raw broccoli sprouts naturally solve this problem by providing both pieces together.
Broccoli sprouts get so much attention because of their high concentration of glucoraphanin. Young sprouts can contain tens of times more glucoraphanin than mature broccoli heads, making them an unusually dense dietary source of sulforaphane potential.

Growing broccoli sprouts at home is surprisingly simple, and the payoff is outsized.

Above are some of the types of sprouting jars available on Amazon.
A note on sprouting jars. For years, we have had a favorite sprouting system that features a tower setup, where water is poured into the top and drains into the other chambers. This allows the young sprouts to get plenty of aeration and prevents overcrowding. A similar stainless steel model is now available (top left photo), and since our decade-old sprouting system is plastic, we have just ordered one.
Sprouting broccoli is a great thing to do in the winter, as it is all done indoors and requires no special tools. Start with good organic seeds, which are readily available and modestly priced online. Start by soaking one to two tablespoons of organic broccoli sprouting seeds, which are easily obtained online, in a wide-mouth mason jar, covering them with cool water and letting them sit for six to twelve hours. Overnight works perfectly.
After soaking, drain the water completely, rinse the seeds with fresh cool water, and drain again. The easiest option at this point is to use a sprouting jar or setup, but if you don’t have one, a wide-mouthd mason jar will do. Just set the jar at a slight angle in a bowl so excess moisture can escape. This balance of moisture and airflow is key; sprouts want hydration, not stagnation.
Over the next three to five days, rinse and drain the seeds two to three times daily, keeping the jar in a dark, cool spot such as a kitchen cabinet. During this short window, the seeds undergo a dramatic transformation. As they sprout, broccoli seeds generate exceptionally high levels of sulforaphane, a sulfur-containing compound linked in the research literature to cellular detoxification, reduced inflammation, improved insulin sensitivity, and activation of the body’s own antioxidant defenses. Gram for gram, young broccoli sprouts can contain many times more sulforaphane than mature broccoli heads, making them one of the most nutrient-dense foods you can grow on a countertop.
Around day four or five, you can move the jar into indirect sunlight for a few hours if you’d like the sprouts to green up and develop chlorophyll. This step isn’t strictly necessary for nutrition, but it does add color and a fresher flavor. The sprouts are ready to harvest once they reach about an inch in length and have tiny green leaves. Give them a final rinse, drain thoroughly, and dry them gently on paper towels before storing. Once harvested, broccoli sprouts keep well in a sealed container in the refrigerator for up to five days.
Broccoli sprouts are best eaten raw or added to foods after cooking, since heat can reduce their benefits. They can be sprinkled onto eggs, salads, soups, grain bowls, or sandwiches, much like a fresh herb or garnish. Pairing them with a little fat, such as olive oil or eggs, and even a small amount of mustard or mustard seed can help your body make better use of their protective compounds.
Grown this way, they deliver fresh enzymes, bioavailable micronutrients, and potent phytonutrients with almost no effort, no soil, and no special equipment; a rare example of food that is both humble and genuinely powerful.
| DR. ROBERT W. MALONE JAN 30 |






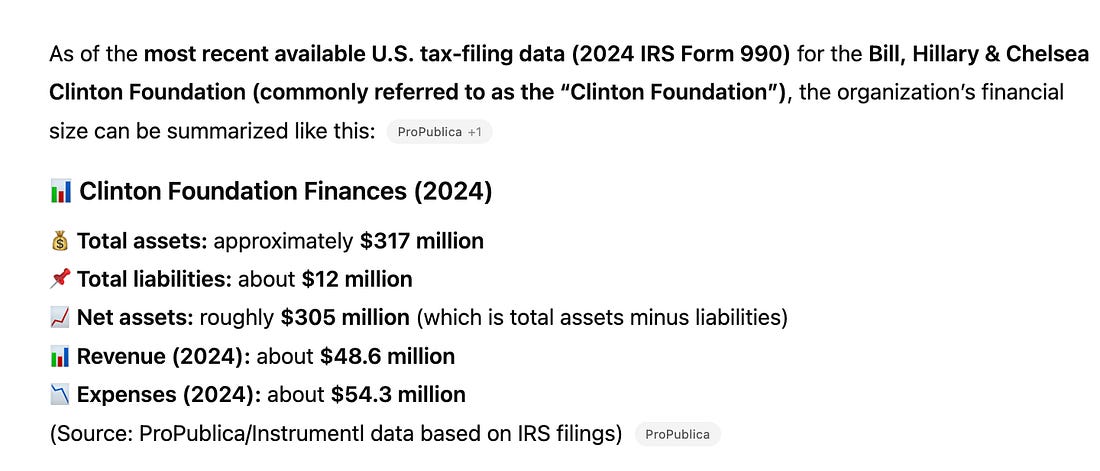
How this all relates to Clinton and the Epstein probe:
In its Jeffrey Epstein probe, the House Oversight Committee chairman sought sworn testimony and documents from Bill Clinton concerning the nature, frequency, and purpose of his contacts with Epstein, including travel records, calendars, correspondence, and any Clinton Foundation records reflecting Epstein-linked meetings or donations.
From Hillary Clinton, the committee requested testimony and records focused on institutional oversight, including whether Epstein or his associates had access to the State Department, and sought emails, visitor logs, and related records to assess how Epstein maintained elite access and whether federal agencies failed to properly scrutinize or restrict him.
None of this has been forthcoming…





I still don’t drink Bud – but it brought a tear to my eye.

On Monday, February 2, 2026, the groundhog will acknowledge the ice,
stress that it is “complex,” “systemic,” and “not new,”
and will assure the public that experts are aligned.
Then he must convene a task force to study it.
After six weeks of hearings, a press conference, and a strongly worded statement about equity for shadows,
he concludes the future was frozen,
but good news: the ice is historic, unprecedented, and someone else’s fault.
He will then go back underground to draft the narrative.
Working to control the messaging, until spring becomes a misinformation problem.

Malone News is a reader-supported publication. To receive new posts and support our work, consider becoming a free or paid subscriber.
Thanks for reading Malone News! This post is public so feel free to share it.
You’re currently a free subscriber to Malone News. For the full exp
| DR. ROBERT W. MALONE JAN 25 |
Having spent the last two days preparing for the worst, we ended up with 2 inches of snow and some cold, wet rain…
Luckily for us, this storm was measured in “man” inches.
(However, the horrifically cold forecast for the next week is not going to be a fun time, but at least we aren’t battling one-degree temps and two feet of snow!)
On one side, we have the Antifa radicals wanting to commit violence, even murder, against Federal officials.
Such as this perfectly normal person:
Before becoming an Antifa (or is that Trantifa?) influencer, urging others to kill ICE agents, Kyle Edward Wagner was a cross-dressing activist.
Yep.. this is the same (sane?) person…
How does one go from cross-dressing weirdo to Antifa radical – all in the name of “protecting” illegal aliens?

The left hive-mind lives in a bizarro world –
Examples of the left threatening to kill ICE agents are everywhere on social media. The violence isn’t coming from the right – let’s be clear
Some of the crazy radicals have millions of followers. One can only hope that the FBI or the DoJ will soon be knocking on their door!

(Then the question arises, why hasn’t this guy been arrested yet?)
Waiting…

On the other side are ICE officials. They are minimally trained to deal with violent crowds or SWAT team methodology (why would they be). These officials are being thrown into situations where they are being doxed, their license plates tracked, the personal information being shared with radicals like the men threatening to kill Federal officials in the video above. The well-funded, financially backed by Soros left has even built apps to follow and track ICE agents.
Ice agents are minimally trained in how to deal with crowds of people threatening them with guns, throwing rocks, screaming, etc. How do ICE agents train for online videos that promote killing Federal ICE agents?
This is the type of behavior that these agents have to cope with.

These are actual cannibals „protesting” on the streets of Minneapolis. Authorities forced the perpetrator to cough up the remains of the finger, but it appears to be too damaged to be reattached.
BTW- this is all being planned and coordinated from the top levels of NGOs run by democrat party leaders and Soros.
City and state officials in MN, rather than cooperating with Federal officials to help find ILLEGAL aliens, are working to cause riots and mayhem. They are encouraging violence and mob action.
Under President Trump, illegal aliens are being given due process while being housed in Federal buildings before being deported. What a shock- under President Trump, ILLEGAL aliens aren’t just being released back into communities.
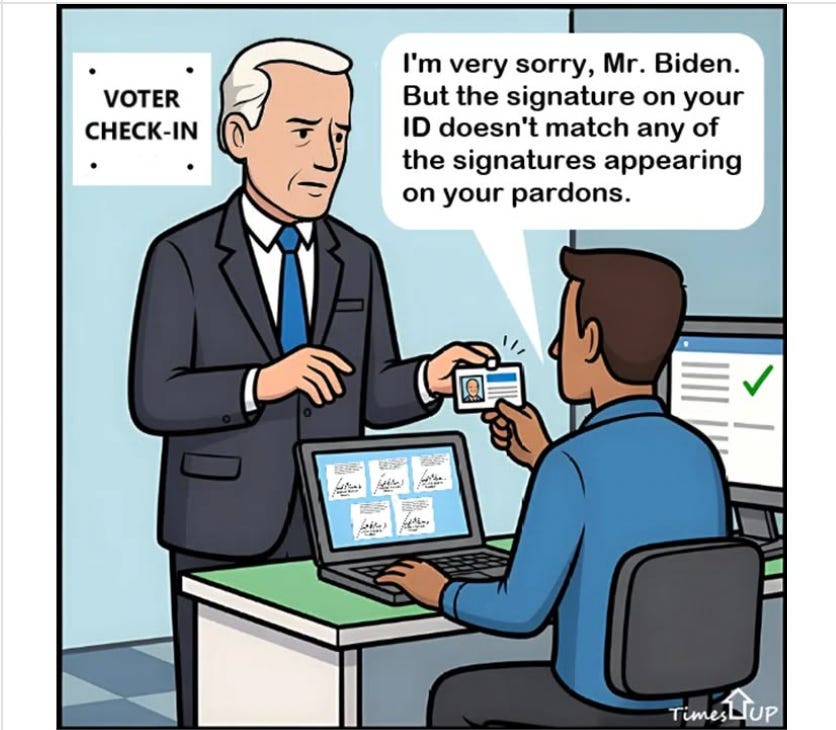
Did you know that under past presidents, illegals would be arrested and “processed” – that is, they would be assigned their own personal attorney, who would then schedule a court date -often years in advance, and these illegals would be RELEASED back onto the streets. Only to disappear from the system again. Rinse and repeat. They have been trained not to carry ID, don’t admit to which country they came from, and basically, were allowed to re-enter the USA to live as they please.
Well, times have changed.
My support and prayers go out to those brave ICE agents who are having to put up with so much abuse and harassment.





Malone News is a reader-supported publication. To receive new posts and support our work here and elsewhere, consider becoming a free or paid subscriber.
Thanks for reading Malone News! This post is public so feel free to share it.
And now for something completely different.

CPR w USA to Cardiopulmonary Resuscitation, co po polsku oznacza resuscytację krążeniowo-oddechową
============================
| DR. ROBERT W. MALONE JAN 23 |


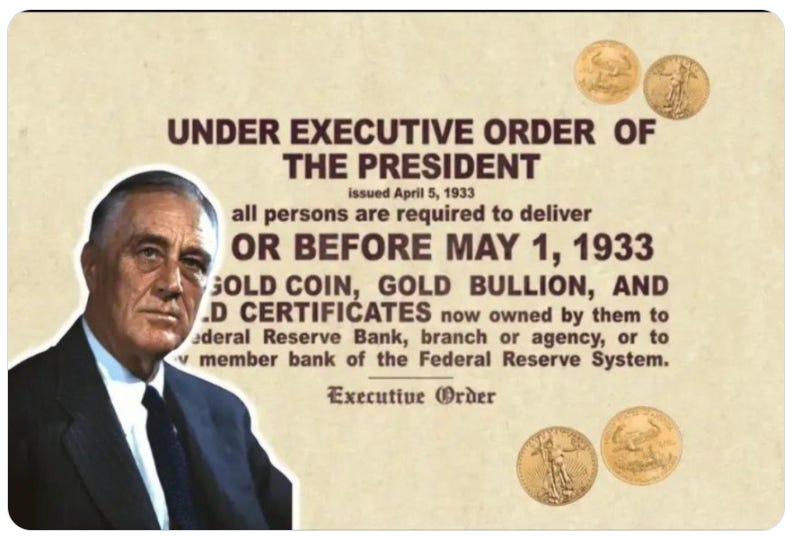
Never forget – the real slavery these days is debt.

Between Gov. Spanberger’s executive actions on day one of her term this week and the bills being presented by the completely blue-dominated legislators in both the state House of Representatives and Senate, Californication is coming at Virginia fast!

As we all watch Virginia descend into an evil maelstrom of Marxist pro-criminality, please allow me to explain what happened and what the remedy is.
Think back to 2024. One of the major reasons the American people elected Donald Trump was so he would fulfill his campaign promise of reducing the size, scope and power of the evil Leviathan housed in the federal administrative state that controls our daily lives in a grotesquely unconstitutional manner.
This necessarily meant greatly reducing the number of federal civilian employees.
As someone who has spent many years in military uniform supervising civilian federal employees, I can assure you that 95% of those civil service employees completely and utterly disregard the fact that their boss is the American electorate.
So when the American electorate says “We think your job equals tyranny and we don’t want you employed in that job anymore,” instead of recognizing that the only people entitled to make this decision are the American voters, they resist, thinking that they are somehow more important than the Constitution and the electorate.
It just so happens that the great majority of these unrepentant federal workers reside in Northern Virginia. So when Trump did what the American people wanted him to do and he fired so many of these unneeded leeches, those unionized leeches decided to vote Democrat at all costs, as a matter of preserving their wholly unnecessary jobs and cushy livelihoods.
Another key fact is that the suburban areas of Northern Virginia like Fairfax and Loudon Counties control state-wide elections, and federal workers control those counties. So the inevitable happened and those unneeded, rent-seeking federal workers swung control of Virginia to Democrats.
And guess what? Those elected Democrats took opposition to reducing the size of the federal government as a mandate to rapidly enact an Orwellian set of laws that would make Karl Marx and Che Guevara blush: outrageous taxation; elimination of basic human rights like those embodied in the Second Amendment; pro-illegal alien policies; refusal to enforce federal immigration laws; draconian rules mandating that confused children can destroy their genitals without parental consent; laws supporting criminality; and a host of other insane laws and policies designed to turn Virginia into a modern version of Ingsoc.
Who is to blame for this evil? Federal workers. Their refusal to acknowledge the will of their boss (i.e., YOU, the American voter) has tossed an entire state into Marxist despair. The ability of federal civil “servants” to cling to their cushy, unneeded jobs is why Virginia has become an un-American hellscape overnight. They simply DO NOT CARE that their fellow Americans are condemned to live in crime and tyranny, because that preserves their cushy sinecures. They are not civil “servants.” They are civil MASTERS, and they don’t care what you think.
Place the blame where it belongs. Federal workers did this to you, Virginia. THEY are to blame.
But there are two ways Trump can remedy this dire state of affairs:
1. Keep on cutting the bloated federal Leviathan.
2. Move federal agencies out of DC and spread them across the rest of the country, depriving this unionized cabal of unelected bureaucratic tyrants of the nefarious power of concentration.
I have a message for Virginia (less Fairfax and Loudon Counties): the rest of America is here to save you. Hold fast, don’t give up, and we WILL eventually save you from this tyranny.
MAGA. MVGA.




Immigration and Customs Enforcement (Urząd Imigracyjny i Celny), zajmującą się egzekwowaniem prawa imigracyjnego i celnego, oraz międzynarodowy skrót In Case of Emergency
===============================================================


TRUE STORY»>





I went to the grocery store yesterday morning… Seriously? The shelves were already emptied of staples.
The storm coming our way is bad, but the ice storm following is going to knock out lots of power. Then what is worse is the temps falling to 1 degree at night and not going above freezing during the day for as long as they can forecast out. With nighttime temps ranging from one to ten degrees night after night. Stock tanks soon become blocks of ice.
In Virginia, our waterlines and back-up systems aren’t built to withstand these temperatures.
So stay tuned – lots of whining is forecast for the coming weeks.
[proszę, by ktoś przetłumaczył to za pomocą programu, ale poprawione, oczywiście. Bardzo ważne, nieznane. Mirosław Dakowski]
| DR. ROBERT W. MALONE JAN 20 |
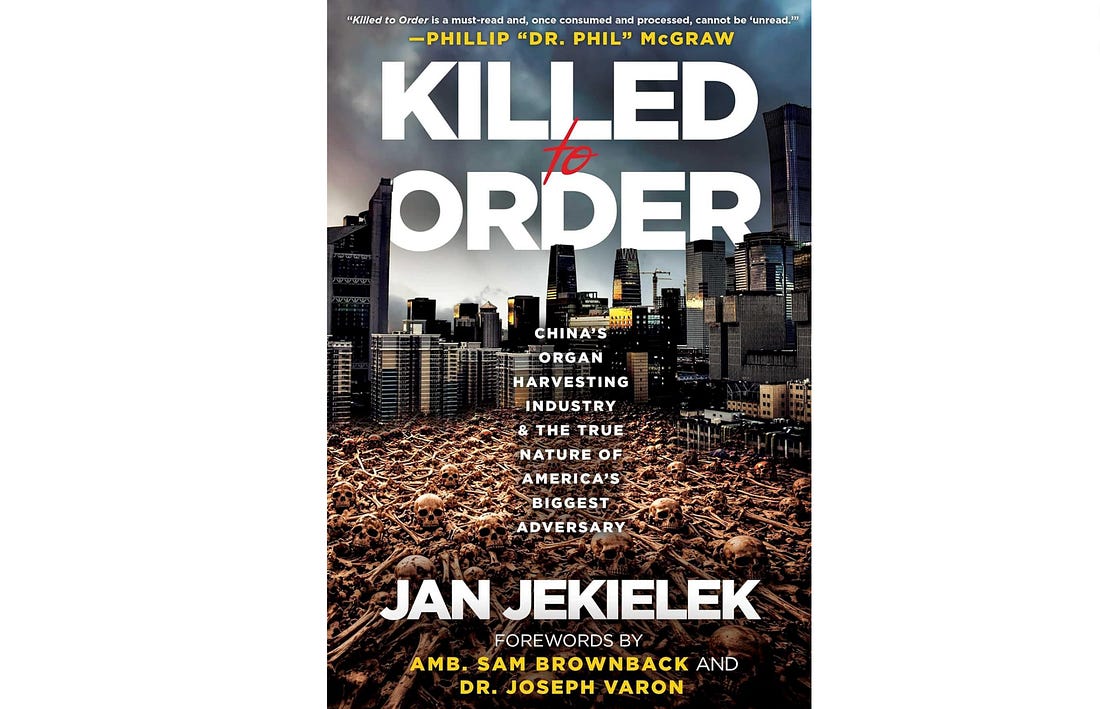
China’s Organ Harvesting Industry and the True Nature of America’s Biggest Adversary
The existence and normalization of forced organ harvesting from living donors is a hard thing for anyone raised on Judeo-Christian ethics to confront, let alone those trained in the medical bioethics developed since the Nuremberg trials. In this book, author and Epoch Times Washington Bureau Chief Jan Jekielek, famous for the “American Thought Leader” interview series, slowly and carefully walks the reader down a path paved with specific examples, making it impossible to look away and avoid the truth of the crimes against humanity that have been normalized by the Central Communist Party of China (CCP).
But that is really just the prelude, a point of entry to the central journey that forms the backbone of this book. By examining this specific set of crimes, the creeping complicity of the western transplant community and the academic and pharmaceutical industry that has enabled them, Jekielek reveals the intentional weaponization of corrupt practices by the CCP as one key component of its policy of unrestricted warfare against the United States, the ultimate consequences of utilitarian ethics applied to public health, and the hidden hand of the CCP in advancing globalist policies by the World Health Organization.
The work starts out by focusing on the horrors of organ harvesting, but the real reason this is a must-read is the moral, logical, and political clarity of its critique of the naïve, corrupt bargain lying at the heart of Kissinger’s China doctrine.
“Killed to Order”, set for publication by Skyhorse and currently available for pre-order on Amazon, exposes the Chinese Communist Party’s (CCP) forced organ harvesting industry. The book draws on survivor testimonies, evidence, and analysis to argue that the CCP systematically murders prisoners of conscience—primarily Falun Gong practitioners, but also Uyghurs, Tibetans, and Christians—for organs on demand, serving both as persecution and a profit-driven tool for elite longevity.
Structured in two parts, the book first details the history, mechanisms, and evidence of this “new form of evil” under communism, including how the CCP instrumentalizes society and makes complicity widespread. The second part explores global implications, such as unrestricted warfare, transnational corruption, and why the U.S. must confront China as its greatest adversary.
The prologue illustrates the issue through a fictionalized story of a Western patient unwittingly benefiting from a “China option” transplant, later realizing its horrific source. Initial reviews include praise from human rights experts, historians, and China analysts, emphasizing the book’s role in highlighting ongoing atrocities and calling for action.
The book opens with Jekielek’s personal journey into the issue, sparked by a 2006 rumor of a secret concentration camp in Sujiatun, China, where Falun Gong practitioners were allegedly held for organ extraction. He interviews “Annie,” the ex-wife of a neurosurgeon involved in the operations, who describes an underground facility holding thousands for live harvesting. Corneas, kidneys, livers, and skin are removed from living victims, with bodies incinerated to erase evidence. A veteran military doctor corroborates this, revealing 36 similar camps across China, treating detainees as “economic assets.” The prologue sets the tone: this is an industrial-scale “kill-to-order” system enabled by the CCP’s persecution of Falun Gong since 1999, when Jiang Zemin labeled it an “evil cult” and vowed its elimination. Jekielek highlights the psychological barrier to believing such horrors, drawing parallels to Holocaust denial, and introduces the “China option” as a euphemism for sourcing organs from prisoners of conscience.
The prologue to Killed to Order frames the horror of forced organ harvesting from the living by placing the reader into the lived reality of the thousands of Western patients facing the grim reality of modern organ matching lotteries. With empathy, the author walks us through the logic of medical tourism-based transplantation, and then introduces readers to the horror of the epiphany that the seemingly miraculous abilities of Chinese transplantation centers to acquire recipient-matched organs depend on maintaining a population of captive living human beings to be organ harvested on demand. It then reveals an even darker underlying reality; having developed this capability and infrastructure, China’s ruling party is now exploiting prisoner organs to advance the lifespan of aged oligarchs. The author’s overall assessment is both starkly blunt and deeply humanitarian, and sets up the body of the work:
There are still many unanswered questions about China’s forced organ harvesting industry. Questions with grave implications for the future of medicine, the future of morality, and the future of the free world. But thanks to the tireless work of investigators, reporters, and unbelievably courageous Chinese whistleblowers, we know far more than we did two decades ago. We know for certain that Falun Gong, Uyghurs, and other groups are still being targeted. We know that the Chinese Communist Party will stop at nothing to ensure its own survival. And we know that Western elites and Western media are being steadily co-opted—made complicit in the CCP’s crimes against humanity.
At the end of the day, that is what this is: a crime against humanity, and we must not allow ourselves to forget the human element.
The body of the text is divided into two sections: Part I: A New Form of Evil, and Part II: The Global Implications of China’s Forced Organ Harvesting Industry.
Part I of “Killed to Order,” titled “A New Form of Evil,” exposes the Chinese Communist Party’s (CCP) systematic forced organ harvesting as an industrialized form of genocide rooted in totalitarian control. Beginning with whistleblower accounts like “Annie’s” revelations of secret camps where Falun Gong practitioners are held for live organ extraction, it traces the CCP’s long history of mass killings under Mao and beyond, illustrating how the regime instrumentalizes healthcare, law enforcement, and society to dehumanize and exploit targeted groups such as Falun Gong adherents, Uyghurs, Tibetans, and Christians. Through survivor testimonies, like Cheng Pei Ming’s harrowing escape after partial organ removals, and a timeline of mounting evidence from reports like Kilgour-Matas and the China Tribunal, the section analyzes why communist systems—especially the CCP’s “regionally administered totalitarianism”—foster such horrors by prioritizing Party supremacy, incentivizing complicity, and viewing human lives as resources for profit and elite longevity.
Chapter 1: A Rumor Is So Extreme It’s Hard to Believe
This chapter delves into the initial investigations following the Sujiatun allegations. Jekielek recounts early reports from The Epoch Times, including Annie’s testimony about her husband’s role in removing corneas from living Falun Gong practitioners. The facility reportedly held up to 6,000 detainees at its peak, with medical teams conducting compatibility tests and providing minimal sustenance to keep organs viable. Bodies were incinerated on-site. A second whistleblower, a military doctor from Shenyang, describes a network of camps where executions are botched to allow live extractions, and families receive fake ashes. The chapter explores the psychological denial of such atrocities, comparing it to initial skepticism about the Holocaust, and introduces key investigators like David Kilgour and David Matas, who later confirm the rumors through their 2006 report.
Chapter 2: A Long History of Killing
Jekielek traces the CCP’s history of mass killing, from Mao’s Great Leap Forward (1958-1962), which caused 45 million deaths through famine and executions, to the Cultural Revolution (1966-1976), where ideological purges killed millions. The chapter argues that forced organ harvesting is a continuation of this pattern, evolving from political campaigns to industrialized murder for profit. It highlights how the Party’s utilitarian ethic—where individual lives are subordinate to collective goals—enabled such systems, with early organ extractions from executed prisoners dating back to the 1980s.
Chapter 3: The CCP Instrumentalizes Everything
Here, the focus is on the CCP’s total control over society, where every institution serves Party ends. The chapter discusses the “610 Office,” created in 1999 to eradicate Falun Gong, coordinating arrests, torture, and organ harvesting. It explains how the regime instrumentalizes healthcare, turning hospitals into extensions of state repression. Blood tests and medical exams in detention centers are not for health but for organ matching, creating a “living organ bank.” The system profits hospitals, doctors, and officials, with transplants generating billions.
Chapter 4: What Targeting Falun Gong Reveals about the Nature of the CCP
Falun Gong, a spiritual practice blending qigong exercises with moral teachings of truthfulness, compassion, and forbearance, grew to 100 million practitioners by 1999, alarming the CCP. Jiang Zemin saw it as a threat to Party supremacy, labeling it an “evil cult” and launching a genocide. The chapter reveals how the persecution provided a “supply” for organ harvesting: practitioners’ healthy lifestyles (no smoking, drinking) made them ideal donors. It details torture methods to force renunciation, and how refusals led to organ extraction. Experts like Ethan Gutmann estimate 65,000-100,000 deaths annually.
Chapter 5: The Evidence and the Road to Get There
This is the evidentiary core, chronicling two decades of proof. It opens with Cheng Pei Ming’s story, the first known survivor: arrested for practicing Falun Gong, he was tortured, blood-tested, and operated on without consent in 2004 and 2006, losing part of his liver and lung. He escaped and confirmed the removals in the US in 2020. The chapter lists a timeline of evidence: 1984 regulations allowing prisoner organ use; 1994 Uyghur extractions; 2005 short wait times for hearts; 2006 Sujiatun revelations and Kilgour-Matas report; 2009 “Bloody Harvest” book estimating 40,000+ transplants; 2012 “State Organs” essays; 2014 “The Slaughter” by Ethan Gutmann (65,000 deaths); 2016 update projecting 60,000-100,000 annual transplants; 2017 Korean hidden camera exposé; 2018 COHRC report on hidden volumes; 2020 China Tribunal judgment of crimes against humanity; 2021 UN experts alarmed; 2022 GRC advisory; 2024 DAFOH report; 2025 Robertson thesis on “extractive repression”; and more. It emphasizes falsified data, short waits, and whistleblowers.
Chapter 6: Why Communist Systems—and the CCP in Particular—Enable Forced Organ Harvesting
Communist systems, especially the CCP’s “regionally administered totalitarianism” (RADT), incentivize atrocities through top-down directives and local competition. The chapter draws on experts like Chenggang Xu (RADT model), Harrison Koehli (pathocracy and “ponerization,” where psychopaths rise), and John Lenczowski (operational communism over belief). The CCP dehumanizes groups like Falun Gong, enabling mass incarceration, database building, and kill-to-order harvesting. It discusses how the system expanded to infants via surrogacy and state seizures, and how Western media shifted post-2001 Jiang Zemin interview to echo “cult” rhetoric.
Chapter 7: Make Everyone Complicit—Including Your Adversaries
The CCP’s “rob, replicate, replace” model exploits Western greed, capturing elites through economic entanglement. The chapter critiques the Kissinger Doctrine for enabling China’s rise, detailing how US financial elites listed state-owned enterprises with minimal oversight, leading to $7-12 trillion in transfers. It argues the CCP wages “people’s war” via fentanyl, elite co-option, and moral compromise, making adversaries complicit in its crimes.
Part II of “Killed to Order,” titled “The Global Implications of China’s Forced Organ Harvesting Industry,” examines how the Chinese Communist Party’s (CCP) organ harvesting atrocities reveal its broader strategy for global dominance, viewing the United States as a zero-sum adversary in an era of “unrestricted warfare” that weaponizes economics, psychology, law, and technology through tactics like the “Three Warfares” and the United Front Work Department as a “magic weapon” for co-opting elites, suppressing dissent transnationally, and corrupting institutions such as the WHO. It critiques America’s “fatal attraction” to the CCP through misguided policies like the Kissinger Doctrine, which enabled economic entanglement and moral compromise, while exploring opportunities for internal change in China via movements like Tui Dang and urging legislative actions, such as U.S. bans on organ tourism and international tribunals, to combat these evils and prevent the erosion of Western values.
Chapter 8: Zero Sum—How the CCP Perceives America
The CCP views the US as its primary adversary in a zero-sum world, pursuing dominance via “Unrestricted Warfare” and “Gross National Power.” Drawing on Pillsbury’s “The Hundred-Year Marathon,” it details covert strategies to weaken America through trade, technology theft, and ideological subversion.
Chapter 9: Unrestricted Warfare (and The Three Warfares)
“Unrestricted Warfare” doctrine weaponizes everything—cyber, economic, legal, psychological. The “Three Warfares” (public opinion, psychological, legal) are detailed, with examples like TikTok as psychological warfare and WTO manipulation as legal warfare. Military-civil fusion ensures civilian tech serves military ends, e.g., Wuhan lab research.
Chapter 10: The Magic Weapon
The United Front Work Department (UFWD) co-opts elites, diaspora, and institutions. It details “Chinese police stations,” transnational repression against Falun Gong media like The Epoch Times and Shen Yun, and smear tactics against survivors like Cheng Pei Ming.
Chapter 11: Transnational Cooperation, Corruption, and Coercion
The CCP influences global bodies like the WHO, exploiting shared technocratic views. It details Huang Jiefu’s partnerships with TTS and Vatican endorsement, enabling abuses. Western complicity in transplants normalizes CCP ethics.
Chapter 12: Fatal Attraction: How the US Perceives the CCP
The US misperceived the CCP as reformable, financing its rise via Kissinger Doctrine. Theories like Smith’s “Thirty Tyrants” argue elites were captured. Decoupling trade from human rights empowered the regime, leading to dependencies in rare earths, medicine, and more.
Chapter 13: Opportunity for People in China?
Change from within is hard due to totalitarianism. The Tui Dang movement—over 455 million renunciations—offers quiet dissent. China’s middle class erodes amid property collapse and inequality, weakening the regime’s “prosperity for compliance” pact.
Chapter 14: Legislating Against Evil
Six US states ban reimbursing China transplants; federal bills like Falun Gong Protection Act and Stop Forced Organ Harvesting Act advance. Institutional reforms (e.g., HHS penalties) and legal theories (e.g., prosecuting organ tourism) offer paths forward. Grassroots action is key.
Epilogue: It’s Not Too Late
Jekielek distinguishes the CCP from Chinese people and culture, arguing the Party’s crimes are anti-China. He warns CCP ethics erode Western morals via medically assisted death and loosened donor rules. The epilogue calls for recovering moral clarity to counter communism’s advance, emphasizing it’s not too late to act.
In Killed to Order: China’s Organ Harvesting Industry and the True Nature of America’s Biggest Adversary, Jan Jekielek delivers a searing, meticulously documented indictment of one of the most horrifying crimes of our era: the Chinese Communist Party’s systematic, state-sponsored forced organ harvesting from prisoners of conscience, primarily Falun Gong practitioners, but extending to Uyghurs, Tibetans, Christians, and others.
Through survivor testimonies like that of Cheng Pei Ming—the first confirmed survivor of partial live organ removal—whistleblower accounts, a comprehensive timeline of evidence spanning two decades (from the 2006 Sujiatun revelations to the 2020 China Tribunal judgment and beyond), and incisive analysis of CCP ideology and global strategy, Jekielek transforms what many once dismissed as an “unbelievable rumor” into an undeniable reality.
What elevates this book beyond mere exposé is its bold framing: forced organ harvesting is not an isolated atrocity but the ultimate lens through which to understand the CCP’s true nature—its dehumanizing utilitarianism, total instrumentalization of society, and zero-sum worldview that treats human lives as disposable commodities for elite profit, longevity, and power. In Part I, Jekielek unflinchingly traces the historical precedents of communist mass killing and explains why such systems enable industrialized murder on demand. Part II expands the scope masterfully, revealing how the regime’s “unrestricted warfare,” United Front co-option, and transnational corruption have entangled the West, making adversaries complicit while eroding moral clarity.
Compelling, urgent, and unflinching, Killed to Order stands as a vital wake-up call, blending rigorous journalism with moral urgency. It challenges readers—especially in the free world—to confront uncomfortable truths, reject normalization of the CCP, and support legislative and ethical countermeasures before these horrors further metastasize.
In an age of moral relativism and geopolitical complacency, Jekielek’s work is essential reading: a beacon of truth that reminds us it is not too late to act, but the window is closing. Highly recommended for anyone concerned with human rights, global security, and the defense of fundamental human dignity.
| DR. ROBERT W. MALONE JAN 18 |

Malone News is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
Thanks for reading Malone News! This post is public so feel free to share it.
You’re currently a free subscriber to Malone News. For the full experience, upgrade your subscription.
| DR. ROBERT W. MALONE JAN 16 |
“The Persians – A History of Iran”
We recently watched an excellent documentary on Iran. The first two episodes on the history up to the 20th century are particularly good, and would be excellent as a primer on Persia for older children. We thoroughly enjoyed watching it and highly recommend. Family friendly. The last episode gets a bit woke though.
( An image of the series is below – we found it on Amazon and the BBC channel):






Malone News is a reader-supported publication. To receive new posts and support my work here and elsewhere, consider becoming a free or paid subscriber.
Thanks for reading Malone News! This post is public so feel free to share it.


Dr. Nisha Verma is an OB/GYN. She’s a professor at Emory. She is trained to manage pregnancy and delivery.
She also could not answer a basic question from Senator Josh Hawley on whether men can get pregnant.
These are the people trying to erase women. Who use terms like people who menstruate.






If you enjoy Malone News, share it with your friends and earn rewards when they subscribe.
| DR. ROBERT W. MALONE JAN 9 |






Thanks for reading Malone News! This post is public, so feel free to share it.









Malone News is a reader-supported publication. To receive new posts and support my work, consider becoming a free or paid subscriber.
| DR. ROBERT W. MALONE JAN 4 |

It all depends on whose ox is being gored.

Estimates of widespread weight loss (around 25 pounds per person) are tied to the prolonged economic and food crisis during Maduro’s illegal reign.

Liberals took to the streets of New York, Chicago, Philadelphia, Washington, and other “blue zones” around the USA as well as the world, to protest the capture of Maduro.
The Democratic Party is defending a ruthless narco dictator, whose reign is known for its massive oppression and starvation. These liberals are protesting for his return to power.

Make it make sense. One day, the Democrats hold “No Kings” rallies; the next, they hold “More Kings” rallies.
The Democratic Party is approaching national political irrelevance.
In the meantime, millions of Venezuelan migrants in the USA and around the world are celebrating in the streets because of the removal of Nicolás Maduro from power.

Personally, I am more than a little disappointed in the statements from Rep. Massie and Rep. MTG regarding the capture of Maduro.
Lots can still go wrong with President Trump’s strategy.
But here is the thing about Trump. He is a master negotiator, and Marco Rubio has turned into one of the best statesmen we have. Together, they can turn the decades-long disaster that is Venezuela into another success story.

Don’t forget, Maduro has given three of our biggest enemies a stronghold in South America. But don’t take my word for it:
China, Russia, and Iran each play distinct but complementary roles in sustaining Venezuela. China has been the regime’s financial backbone, providing tens of billions of dollars in loans repaid with oil, along with telecommunications and surveillance systems that help maintain internal control; today, its role is more cautious and transactional, focused on recovering value rather than ideology.
Russia serves as the key political and military guarantor, offering security cooperation, intelligence support, and diplomatic shielding that helps keep Nicolás Maduro in power during moments of acute legitimacy crisis.
Iran, meanwhile, functions as a sanctions-evasion and operational partner, supplying fuel, refinery expertise, and illicit trade networks that allow Venezuela to keep its energy system running despite international restrictions.
Together, China keeps the state solvent, Russia keeps the regime standing, and Iran keeps the system functioning under sanctions.
Chat-GPT
The thought of China, Russia, and Iran having a stronghold on our southern doorstep should make anyone pause…




Malone News is a reader-supported publication. To receive new posts and support our work here and elsewhere, consider becoming a free or paid subscriber.
Thanks for reading Malone News! This post is public so feel free to share it.
| DR. ROBERT W. MALONE JAN 2∙PREVIEW |


| DR. ROBERT W. MALONE DEC 28 |



Malone News is a daily, reader-supported publication. To receive new posts, make comments, and to support our work, consider becoming a free or paid subscriber.